

Buckraking: Did A Medical Monopolist Buy Off CNN?
Buckraking: Did A Medical Monopolist Buy Off CNN?
Vizient is a little-known company that consolidated control over hospital purchasing and helped induce shortages. Is CNN tolerating chief medical correspondent Sanjay Gupta being on Vizient's payroll?
Welcome to BIG, a newsletter on the politics of monopoly power. If you’d like to sign up to receive issues over email, you can do so here.
Today I’m writing about CNN’s chief medical correspondent Sanjay Gupta and the practice of ‘buckraking,’ which is when journalists do speaking gigs for corporations they cover in return for large amounts of money.

CNN Tells a Partial Truth About Medical Shortages
Over the past three months, one of the biggest stories in American politics was a shortage of baby formula, resulting from the shutdown of a major Abbott plant producing the stuff. There were Congressional hearings, headlines, and the Biden administration ultimately used the Defense Production Act in an emergency decision to fly in formula from Europe and Australia.
Such a crisis is not a one-off. Unfortunately, dealing with a shortage of a critical good is no longer an unusual situation in America. And while most people chalk up shortages to Covid, in fact, brittle supply chains causing a lack of critical goods preceded the pandemic. For instance, hundreds of drugs have been in shortage since the mid-2000s. (The Food and Drug Administration keeps a list, in case you want to know what you can’t get.) The problem is so bad that the FDA has warned that a generation of doctors in the U.S. have not been trained properly because they never have a full suite of pharmaceuticals on hand to practice medicine.
What Covid did was make the problem worse and more obvious, as thinned out production processes snapped all over the place, causing a lack of everything from black pipe for housing to spicy chicken breasts to medical supplies. But shortages have been a pervasive reality for two decades in health care, and they continue and even worsen. So why hasn’t there been a meaningful political approach to stopping shortages? One reason is because important figures in the media are accepting large sums of money from monopolists who cause them.
Let’s start with who is talking to the public about shortages in, say, the medical area. Covid catapulted a host of conflicted media celebrities who had some scientific or medical pedigree into superstars, and these people then explained a version of what was happening to a confused and frustrated nation.
I want to focus on two of them, CNN Chief Medical Correspondent Sanjay Gupta and former Food and Drug Administration Commissioner Scott Gottlieb. Both are savvy and experienced medical professionals, and well-versed in the art of political celebrity. Gupta reports in an authoritative manner about what is happening in medicine, and he became much more important over the last few years as one of CNN’s most respected journalists. Here, for instance, is Gupta reporting about a bad situation in health care, a shortage of contrast dye for medical scans, due to a GE factory located in Shanghai shutting down.

It’s an important problem when doctors nationwide can’t give their patients CAT scans or do other forms of imaging. There are secret stashes of contrast dye that doctors keep that they can use in case they are really desperate. Gupta explains much of this, walking through the problem in easily understandable language, eschewing complex medical jargon. He’s a media pro, and you can see it in the way he talks.
Meanwhile, turn on Bloomberg or CNBC and Gottlieb is making projections, often accurate ones, about important medical questions like how dangerous Omicron would turn out to be. Shortages and a lack of manufacturing capacity were featured in Gottlieb’s important and widely publicized book “Uncontrolled Spread” about preparing for the next pandemic. He will be an important voice in the Republican Party’s approach to public health.
But what neither Gupta nor Gottlieb explain is *why* production of imaging dye is concentrated in one GE factory in China, or why this shortage, like many others in medicine for everything from standard antibiotics to saline solution, have become routine over the past 20 years. It’s not like shortages are inevitable; prior to 1999, the idea of shortages in America was outlandish, something we used to mock as Soviet. And there’s a very interesting possible reason why neither one of these men is laying out the problem, a problem that Gottlieb, at least, understands but has chosen to omit from his recent public commentary.
BIG is a reader-supported newsletter focused on the politics of monopoly and finance. This is journalism and advocacy that challenges power, so please consider a paid subscription. You can always get lies for free. The truth costs a few bucks, but in the long run it’s much cheaper.
Let’s start with the reason for the shortages. Like a lot of problems in health care, it’s caused by middlemen with monopoly power pushing down what producers are paid such that it’s not worth producing. We saw this with baby formula, where a big buyer (often called a ‘power buyer’) - in this case the federal government - structured the market so that there is a monopoly producer, Abbott Labs. (GPOs are involved in baby formula, but to what extent it’s not entirely clear.) When Abbott’s Sturgis factory had to be shut down, the result was a massive shortage.
In hospital purchasing, the ‘power buyers’ aren’t the federal government, but a small number of firms called Group Purchasing Organizations. GPOs are purchasing agents for hospitals, and after a decade of mergers, three of them - Vizient, Premier, and HealthTrust - now manage an estimated $300 billion of hospital purchasing for 5000 health systems (as well as nursing home facilities and other providers), or 90% of hospital supplies in the United States.
Importantly, GPOs are not paid by the hospitals directly, but by suppliers who want to sell to hospitals. While GPOs were created in the early 20th century as purchasing coops for hospitals, today they are for-profit corporations that essentially sell market share to medical supply and pharmaceutical producers who want to get access to the hospital market. The shift was a result of a legal change; in 1987, Congress exempted GPOs from anti-kickback rules, and GPOs then morphed from useful coops to predatory middlemen. (The politics here are odd; GPOs are mostly owned or controlled by a few prestigious wealthy hospitals, while extracting from normal and poorer hospitals.) As a result, GPOs both raise costs in the overall hospital sector, and consolidate supply chains. I wrote up this industry sector up in September.
Like Amazon does to small vendors and third party sellers, GPOs pressure small producers to give them higher and higher administrative fees, ultimately destroying their margins and causing them to either offshore production or use substandard factories that would force a recall or factory shutdown. GPOs also inflates cost: when a small competitor was finally allowed to compete with Tyco (now Covidian) over oximeters, prices dropped by 30%. Some experts put GPO-hospital-supplier cartel cost at $100 billion annually.
Along with higher cost and less innovation, there is also the pooling of production and risk. As Phillip L. Zweig and Frederick C. Blum noted in 2018, one reason the U.S. has been importing saline solution - aka salt water - for years is because GPOs rely “almost exclusively on Baxter for these products.” And Baxter not only didn’t produce enough, causing shortages and thus reliance on imports, but also put its key plants in Puerto Rico, which was devastated by Hurricane Maria. The pooling of production led to pooling of risk.
What GPOs are doing is destroying price signals. Flexible pricing is a great way to create production where it’s needed. A buyer that wants a highly sought after item would offer more money, and eventually production would come online, at least theoretically, because producers want to make stuff they can sell for more money. But if there’s a middleman that controls access to buyers, and that middleman allocates the whole market to one producer that gives them kickbacks, then new producers won’t come online. And if that producer goes down, then you have shortages.
When I wrote this in September, we hadn’t yet seen the baby formula problem, or the contrast dye shortage. But both are a result of exactly this dynamic, power buyers consolidating supply chains, and then the weak link in the chain blowing up. GE, for instance, has more than 50% share for contrast dye in hospitals. When its Shanghai factory went down, there was no way to ramp up production quickly to supply more than half of America’s needs. Its main competitor, an Italian conglomerate named Bracco, has some market share with an equally effective line of products, while Bayer and Guerbet have less than 5% of the market. But none of these competitors can provide enough supply to deal with the hole the GE shutdown caused.
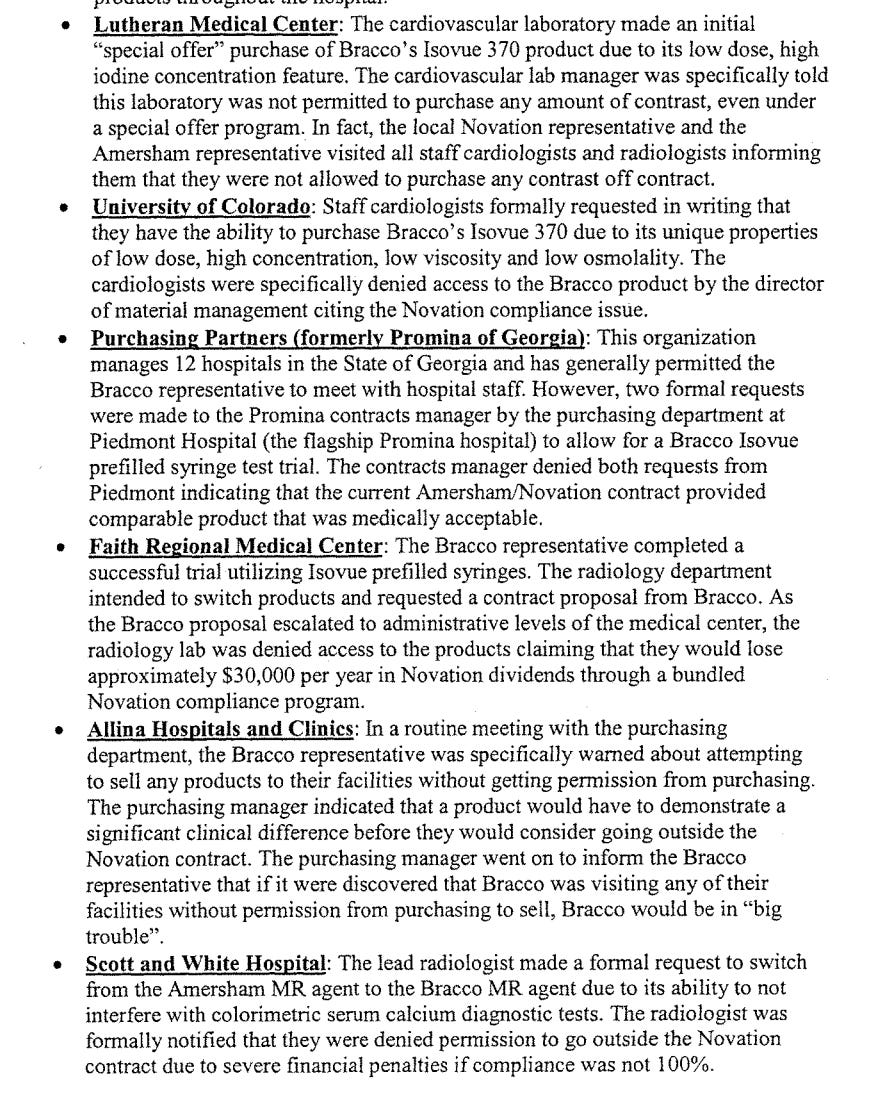
The market for this dye wasn’t always so consolidated. In 2003, each of these four firms had a roughly equal share. But Bracco saw the coming consolidation, and gave a statement to Congress about GPOs locking them out. Robert Aromando, VP of Marketing for Bracco, noted how their salespeople were not even allowed to talk to hospitals by Novation, one of the main GPOs. (Novation is now, after many mergers, called Vizient.) Novation had purchasing contracts with hospitals, and would give hospitals rebates if they bought a certain amount of medical products through its service, and penalize those who didn’t. The University of Utah, for instance, wanted to switch to Bracco products, but they were told that “any attempt to purchase off contract would cause the hospital to forget up to $80,000 per year in discounts on other products throughout the hospital.”
Aromando gave a list of examples of Novation thwarting an open market for contrast dye, which undercut the ability of new firms to enter the market.* The net result was that the market consolidated into two firms, GE (which bought Amersham, one of the producers) and Bracco. Because contrast dye is likely a relatively low margin product, GE offshored its production, and did not have enough extra capacity outside of Shanghai to serve the U.S. likely because there wasn’t enough of a justification for investing in redundancy. The result is a shortage.
The GPO shortage problem is not a secret. The Senate almost closed the key loophole enabling GPO kickbacks in the early 2000s. (Almost, but not quite. We can thank Chuck Schumer for killing that reform). Scott Gottlieb himself testified to the Senate in 2011 on the consolidation of manufacturing as a result of GPOs, and said it even more explicitly to the Associated Press in 2018. In 2019, when he was FDA commissioner, the agency came out with a report fingering the dominant middlemen as a cause of shortages. Dave Dayen made GPOs a chapter of his 2020 book Monopolized, and journalist and advocate Phillip Zweig has been campaigning nonstop against this problem for 20 years.
After Covid made it clear the problem was a matter of national urgency, the Biden administration, in their 100 day supply chain report in June of 2021, noted the exclusive contract arrangements of GPOs that caused shortages and supply chain fragility. Just two months ago, 60 Minutes did a story on shortages, with industry insiders fingering the GPOs directly. FDA Commissioner Robert Califf referenced this story multiple times to Congress in the hearing on baby formula.
So why don’t we fix it? Well, because the GPOs are able to tamp down the criticism. How? Political influence, and money. They were able to get Health and Human Services Secretary Xavier Becerra to remove all references to market power from HHS’s 2022 report on supply chains. HHS has authority to address the problem, but no one in the White House or HHS focused enough to do so.
But GPOs also heavily influence the media, and use that to reduce pressure on government to act. And this brings me to CNN’s Sanjay Gupta, who is likely taking money from corporations he’s supposed to cover as a journalist, in a practice known as ‘buckraking.’ First, the only story I can find on CNN mentioning GPOs is one praising Vizient for its cooperation with the FDA on shortages during Covid. This lack of skepticism is in contrast to CNN’s wonderful work on supply chains in, say, the food sector.
And I have to wonder whether buckraking plays a role. Here’s how buckraking works. Large powerful firms like Vizient host conferences for clients and suppliers. Doing so is standard for corporations and Wall Street, who invite important politicians and policymakers to these events, and pay them lots of money to give speeches. Current Treasury Secretary Janet Yellen, for instance, made millions doing this, and Hillary Clinton’s speaking fees became a bit of a scandal in 2016. But it’s not just politicians, TV journalists like Gupta also take money. According to his booking agent, Gupta’s fee for a speech is somewhere between $150,000-$299,000.
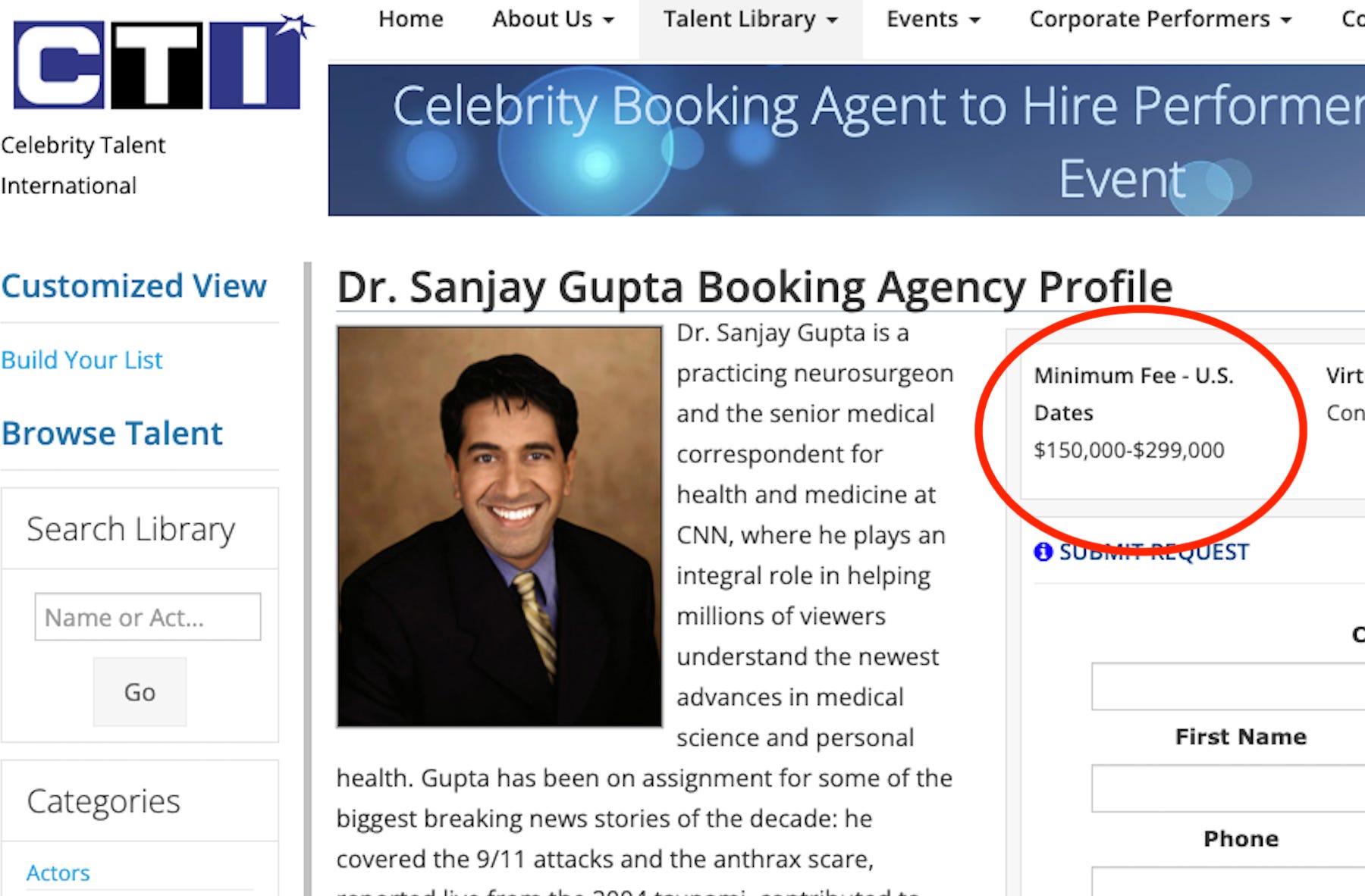
One of Gupta’s likely clients is, surprise surprise, the giant GPO behind the contrast dye shortage, Vizient. Gupta was a keynote speaker for a Vizient conference last year, discussing with Vizient CEO Byron Jobe what would bring “meaningful change” in healthcare. Gupta also spoke at a Vizient conference in 2019. (The connections don’t end there. Gupta teaches at Emory, a major Vizient shareholder facility, and practices medicine at Emory-affiliated Grady Hospital. In 2017, four top Emory executives were on Vizient’s board.)
Now, to be clear, I don’t have evidence Gupta is choosing to report certain stories because of these engagements with Vizient. A lot of things go into editorial choices. And Vizient is probably inviting Gupta because he’s famous, and not necessarily to influence coverage. But it is a conflict of interest. Gupta shouldn’t be seen to be taking money from a powerful middleman supplier in an industry he is supposed to report on.

I asked CNN about Gupta’s speaking fee from Vizient, whether he gave it to charity, and whether it presented a conflict of interest. Here was the response from Neel Khairzada, CNN’s Director of Public Relations.
Mr. Stoller,
Your email was forwarded to me. CNN thoroughly reviews all staff speaking engagements to insure they do not pose any conflicts of interests. CNN does not disclose staff compensation.
Best regards,
Neel
I asked for more info, but that was all I got.
Gupta wasn’t the only keynote. Another famed speaker sitting on the keynote panel discussing ‘meaningful change in healthcare’ was, as it turns out, Dr. Scott Gottlieb, who also does paid speaking gigs. In the case of Gottlieb, he’s not holding himself out as an unbiased journalist - he is on the board of Pfizer after all, so if he’s getting paid it’s not a violation of media ethics, per se.

Still, Gottlieb is widely respected as an authority in these areas, and while he absolutely knows the problem cold and has publicly blamed GPOs for shortages, he has changed his tune. As journalist Dave Dayen noted, “I'm reading Scott Gottlieb's book right now and a search for GPOs yielded nothing.” Given that this book purports to help prepare the U.S. for the next pandemic, it’s a significant missing piece.
Ultimately, media stars in line or not, policymakers in government need to act on GPOs. That means for starters getting data on how exclusionary contracts by these middlemen consolidate supply chains. The FTC has already investigated this dynamic in a number of areas, like dominant middlemen in groceries, and in the adjacent space of pharmacy benefit managers. In addition, Congress needs to take action against power buyers in general and end the exemption that allow GPOs to induce kickbacks. And antitrust enforcers need to revisit their 1996 guidance on health care.
Still, the media has a key role. In a democracy, public knowledge, or public ignorance, really can drive policy. So it’s important to understand why the public isn’t being informed about the problem. If we don’t act to deal with GPOs, then our markets will shrivel, shortages will get worse, our fellow citizens will die, and we will keep wondering why we can’t produce the medicine that we need.
And that’s because Gupta and CNN simply look the other way.
Thanks for reading. Send me tips on weird monopolies, stories I’ve missed, or comments by clicking on the title of this newsletter. And if you liked this issue of BIG, you can sign up here for more issues of BIG, a newsletter on how to restore fair commerce, innovation and democracy. If you really liked it, read my book, Goliath: The 100-Year War Between Monopoly Power and Democracy.
cheers,
Matt Stoller
* Here’s the full list from Aromando’s testimony in 2003 on how Bracco was excluded from the market.
Matt … just observing that given your expression of concern over experts being co-opted for corporate sector gain is it no wonder that trust in technical experts is plummeting. As you know a huge problem in scientific research is the sources of funding of that research. Corporate sources, or even worse dark money funders with unknown corporate backing give that funding with expectations that they will get the results they want. And total research funding is THE measure of success for researchers in higher education … which leads to associated promotion, tenure, salary and prestige, not to mention new positions with bigger labs, more graduate students, etc at a larger institution. So, my GP ( at a MAJOR U.S. health care system) still pushes colonoscopies, blood pressure medications ( high normal readings) and cholesterol medications ( also high normal). GP is young which means either that’s being taught or the hospital system pushes it.
Too much corruption to accept the advice of experts.
Amazing work, thanks for what you're doing.